
|
1A Grange Rd. Toorak 3141 Australia Ph. 9867 6405 |

|
Minimal Intervention Dentistry is all about reducing drilling and preserving as much strong, healthy tooth as possible. Traditionally dentists have treated decay by drilling away far too much sound enamel. The reason is easy to understand. Years ago the only decent filling material was grey, metallic amalgam. It was tough and durable but did not adhere to tooth substance so the only way to keep it in place was mechanically, by locking it into a hollowed out cavity. This undercutting weakened the tooth and sometimes damaged the nerve. Today dentists have the option of using white, adhesive composite resin, so there is no excuse for excessive drilling. Unfortunately old habits die hard. The cavity designs which were advocated a hundred years ago are basically still taught and used today. |
|
DECAY, BETWEEN THE TEETH AND DIFFICULT TO REACH |


|
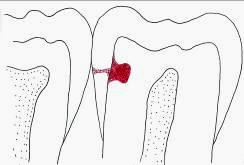
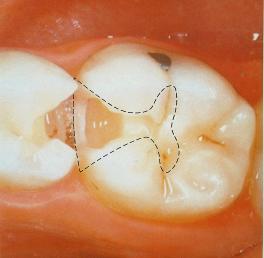
�Here is an illustration. Consider an average, everyday dental decay. This one is at the side of a tooth, where it abuts against its neighbour. It is effectively between the teeth. An X-ray proves it is there but it is hard to spot with the eye. There is no ready access to the lesion since the nextdoor tooth is jammed against it.
|
|
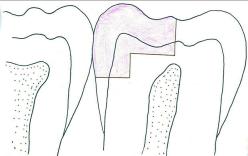
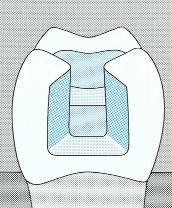
The usual approach is to drill across the biting surface and then sink a trough between the teeth. A great deal of sound enamel is destroyed in the process � in fact more healthy tooth is removed than that which is diseased. |

|
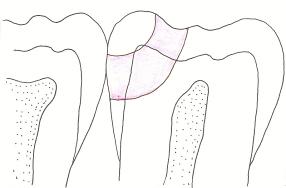
There are better alternatives. Back in 1986 two dentists, a Melbournian and an American, described a clever improvement. They suggested burrowing through the tooth and preserving the edge or marginal ridge. The resultant preparation was virtually a tunnel from the biting surface, through to the decay in the wall of the tooth. Part of the reason this technique emerged was that the new white composite resin materials were proving reliable. These were soft and easily manipulated before setting with exposure to white light. |

|
Unlike the old amalgam, the new composites could readily be worked into the narrow confines of the prepared cavity. This Tunnel Restoration retained much more healthy tooth than previously but it was difficult to perform and never really caught on. |
|
At about the same time other developments were taking place. Another Australian, Graham Craig, began working with silver fluoride solutions and realized that it immediately disinfected the surface of decay and, at the same time, stimulated remineralisation. In other words it killed the bacteria and prompted rehardening. It effectively arrested decay. People find it difficult to imagine decay actually stopping and reversing but this is often seen naturally on the surface of teeth.� If rotting has only begun superficially and diet and cleaning improve, the enamel can often recalcify and take up mineral that was previously lost. The area leaves a tell-tale mark but is like a scar on the skin - tougher and more resistant than it was originally. He suggested simply removing the obvious bad decay in the soft dentine while remineralising the layer underneath by applying silver fluoride. |
|
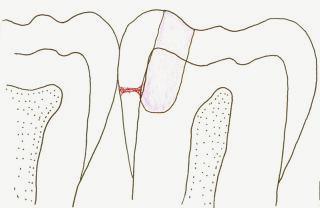
Meanwhile the American, P. R. Hunt, refined the Tunnel Restoration further and argued that, unless the tooth had deteriorated to the point of a physical hole, it was not always necessary to drill through the edge of the enamel wall. This meant the side of the tooth could be preserved as well as just the ridge of the biting surface. .
In 2002 I published an article in the ADA News Bulletin� proposing that the two approaches could be combined. The drilling would merely target the dangerous decay in the central part of the tooth while silver fluoride could be used to kill off any remaining bacteria and help repair the softened enamel at the side. Because the tunnel and the filling stopped short of breaking through the tooth I called it a Terminated Tunnel Restoration. I have practiced this type of filling successfully for over ten years now.� It preserves more natural tooth than with any other design and is quicker and easier for both the dentist and patient. It certainly can not be used in all cases but for moderate sized decay I believe it is the technique of choice. You may like to read up on this approach and the philosophy behind it. The Terminated Tunnel Restoration and The Case For Minimal Intervention Dentistry are published articles. They are written for the profession but they do provide a more detailed insight. The newsletters have some interesting angles too. See World�s Fastest Dentists, Viva La Revolution and Why Fillings Should be White. |

|
THE TERMINATED TUNNEL RESTORATION |
|
When Einstein published his famous paper on relativity over a century ago the immediate response was - almost nothing! Hardly anyone read it. Sometimes new ideas take a while to catch on. In dentistry the design of fillings was established back in Einstein�s early days. The major principle was - drill out the every last hint of decay! As I suggested above, researchers are now showing there are smarter ways of treating cavities than simply drilling. So, are these advances really catching on? Only slowly! In dentistry new ideas can take a very long time to catch on, especially when they challenge long held beliefs. If you think about it, decay is a sort of tooth infection, with germs burrowing into the tooth.� If a foot develops an infection it requires treatment but not necessarily amputation. Infected dentine is likewise a problem but perhaps not all of it needs to be drilled away. |
|
We have known for a while that surface decay often reverses. It is common to see brown spots on enamel, suggesting it has initially softened the changed its mind, usually because diet and cleaning improved and mineral flows back into the surface. These areas of arrested decay are actually tougher and harder than the original enamel. Traditionally dentists believed substantial decay only worsened and they drilled even till the nerve became damaged and the tooth weakened! Lately, the need for such deep drilling has been questioned. Experiments show that if a cavity is sealed with gluey cement and bacteria are deprived of nutrient, the decay simply dies off over time. Glass ionomer cements make fabulous under-coats at the base of fillings. They block plaque nutrients out of the cavity, raise the pH to combat bacteria and release mineral to reharden dentine. In the meantime, the pulp at the centre of the tooth joins in by releasing its own chemicals to further attack the germs and repair damage. All teeth need is a decent, fighting chance against decay. |
|
A CONVENTIONAL FILLING DESTROYS TOO MUCH HEALTHY TOOTH |
|
AN IMPROVED APPROACH |
|
FURTHER IMPROVEMENTS |
|
A COMPLETELY NEW FILLING |

|
The Lotus Formula I cars of Colin Chapman won seven Constructors Titles during the sixties and seventies, regularly defeating bigger, more fashionable companies such as Ferrari. Lotus championed innovation and was the first to place its engine behind the driver (�mid - engined�) for better weight distribution and the first to fully utilise aerodynamics, culminating in the famous �ground effects�. This revolutionary design effectively sucked the car down to the road, due to the partial vacuum generated by air flow trapped under the body. |
|
The concept was eventually banned because it produced such massive G -forces during cornering that drivers nearly blacked out. Probably Chapman�s greatest insight was that power-to-weight ratio could be improved by reducing a car�s weight and that a lighter car would perform and handle better.
|
|
Rather than adding power with larger, heavier engines, he enthused about �adding lightness� to the design. If Chapman had lived on he would probably have approved of today�s Minimal Intervention Dentistry and been horrified by the drilling associated with some crown and porcelain reconstructions.
|
|
MI dentistry seeks to reduce drilling and preserve healthy tooth structure. If a cavity has to be drilled, the dentist should increase the smallness. The principle is to add lightness. |
